




SUMMARY
To examine the relationship between normative and self-perceived treatment need assessed by different measures, comprising two Oral Health-Related Quality of Life (OHRQoL) scales.
This cross-sectional observational study comprised 386 children aged 11–16 years registered for a first consultation at the Orthodontic Department of the University Hospitals of Leuven (Belgium). Normative treatment need was assessed by the Dental Health Component (DHC) and the Aesthetic Component (AC) of the Index of Orthodontic Treatment Need (IOTN). The children completed questionnaires comprising the Child Perceptions Questionnaire (CPQ11–14) and the Oral Aesthetic Subjective Impact Scale (OASIS). They also scored the AC of IOTN themselves. Spearman correlations, Mann–Whitney U-tests and signed-rank tests, a Bland–Altman plot, and an intra-class correlation were used to analyze the data.
Significant, yet weak correlations (maximum ρ = 0.23 for the CPQ emotional well-being domain) were found between normative orthodontic treatment need (IOTN AC) and most of the OHRQoL measures. Similarly, between the IOTN AC scores of the expert and the IOTN AC ratings given by the child a significant correlation (ρ = 0.37, P < 0.0001) was found, but with very poor agreement (95 per cent limits of agreement −4.3, 5.1). For the DHC of IOTN, only a relation was found with the AC child (ρ = 0.20, P = 0.0001).
These results suggest that the commonly used IOTN as a clinical assessment tool for orthodontic treatment need should be reinforced by OHRQoL measures, like the OASIS, expressing patients’ perceived treatment need.
Introduction
Although malocclusion in itself is neither a disease nor a life-threatening condition, there has long been a marked demand for orthodontic care (Jenny, 1975; Mohlin et al., 2002).
Often, the decision for orthodontic treatment is based on a mutual agreement by the clinician in association with the patient and parents (Ahmed et al., 2001).
Considering the health of one’s dentition, it is the dentist who is the most qualified and trained person to notice each occlusal trait likely to undermine its longevity and satisfactory functioning (Shaw et al., 1975). The Dental Health Component (DHC) of the Index of Orthodontic Treatment Need (IOTN) proposed by Brook and Shaw in 1989 is a ‘golden standard’ assessment tool helpful in taking this decision. For patients assigned to the IOTN DHC groups 3 and certainly to groups 4 and 5, treatment is required (Kuijpers and Kiekens, 2005). These especially with regard to future impairments as only few functional indications exist for orthodontic treatment (Brook and Shaw, 1989).
Nevertheless, since the main motivation for many patients who seek orthodontic treatment is an improvement in appearance rather than function, their own perception of dental appearance is of even more importance (Espeland et al., 1993; Wedrychowska-Szulc and Syryńska, 2010). Therefore, any treatment need assessment should at least allow appropriate weighting of the aesthetic aspect of a malocclusion. The Aesthetic Component (AC) of the IOTN has been particularly designed for that purpose (Brook and Shaw, 1989). Nevertheless, the AC of IOTN still being a clinician-based measure has its limitations as it measures normative rather than perceived treatment need. In this study, this has been partially addressed by demanding patients to self-rate their dentition in accordance with the AC of IOTN (Kok et al., 2004). As Becker et al. (1993) define quality of life as ‘a person’s sense of well-being that stems from satisfaction or dissatisfaction with the areas of life that are important to him or her’, malocclusion and orthodontic care have become an oral health-related quality of life (OHRQoL) issue as it impacts the psychological and general well-being of a child (Shaw et al., 1980; Kenealy et al., 1991; O’Regan et al., 1991; Berg, 2001; Rinchuse et al., 2002). Of all the dental treatments studied, the treatment of malocclusion, which has such a large psychosocial component, calls out for the use of OHRQoL measures (de Oliveira et al., 2008). Therefore, in this study, the perceived treatment need was additionally assessed by two OHRQoL indices, the Child Perceptions Questionnaire (CPQ) (Jokovic et al., 2002; O’Brien et al., 2006) and the Oral Aesthetic Subjective Impact Scale (OASIS) (Mandall et al., 1999).
As we observe in orthodontic practice that perceived treatment need not always seems to reflect normative treatment need, the aims of this study were to determine both normative (DHC and AC of IOTN) and perceived treatment need (OHRQoL measures CPQ and OASIS as well as the children’s self-rated AC of IOTN) and to evaluate the relationship between them. The agreement between AC expert and AC child was studied in more detail.
Subjects and methods
Recruitment started from April 2009 to July 2012: every 11- to 16-year-old healthy child registered for a first consultation at the Orthodontic Section of the Department of Oral Health Sciences was kindly asked to participate by completing a questionnaire containing the different perceived treatment need measures. Children who had previous orthodontic treatment and who did not have thorough knowledge of the Dutch language to fully understand the questions were excluded.
The study protocol was approved by the Medical Ethics Committee of the University Hospitals of Leuven (Belgian Number B32220096365, 8 May 2009). Informed consent was obtained from all subjects and one of their parents.
Three hundred and eighty-six children (186 boys and 200 girls) with a mean age of 13.18 years (SD = 1.34) completed the questionnaires. Age and gender were recorded because of their potential associations with both outcome and explanatory variables.
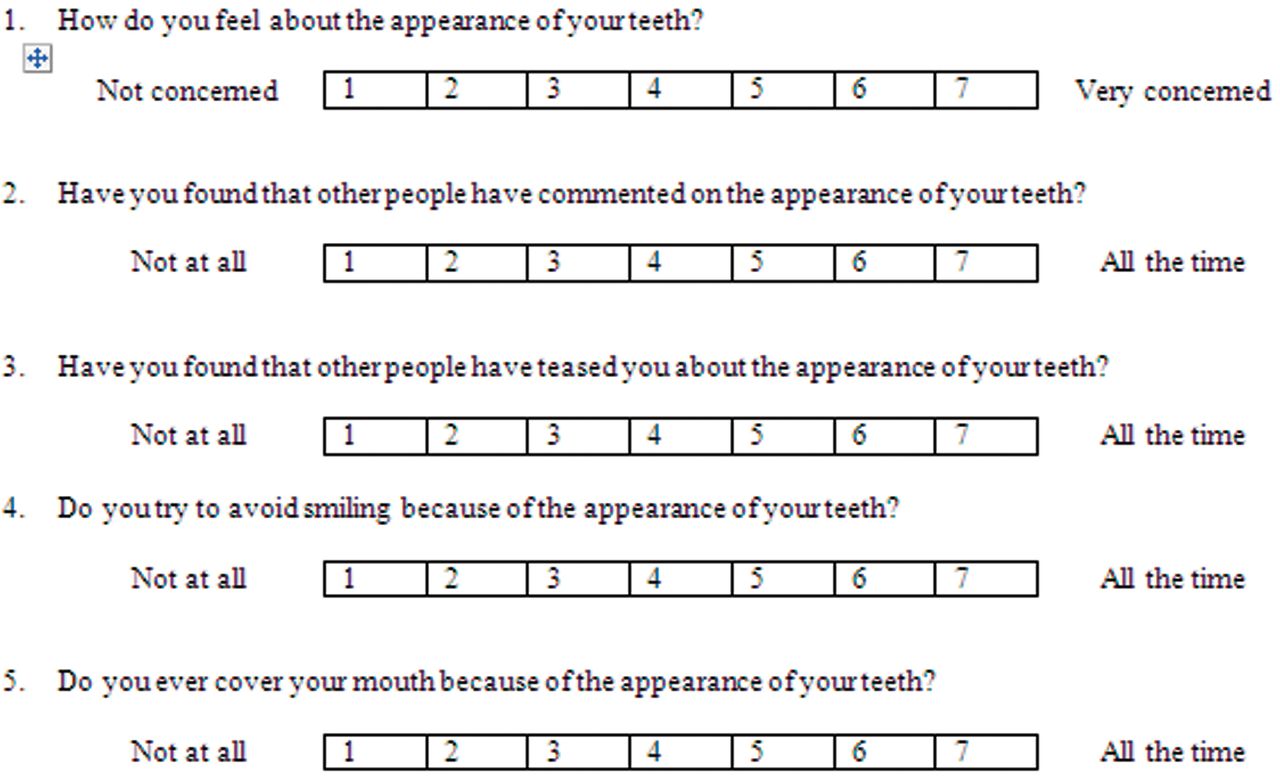
The OHRQoL of the child was scored using the Dutch translation of the CPQ11–14. The CPQ11–14 is an OHRQoL assessment for children aged 11–14 years. It was developed to apply to children with various dental, oral, and orofacial disorders and has been shown to have adequate validity and reliability (Jokovic et al., 2002). The CPQ contains 37 questions about the frequency of events in four domains: oral symptoms (OS), functional limitations (FL), emotional well-being (EW), and social well-being (SW). Each question has five answering possibilities: ‘never’ (scoring 0), ‘once or twice’ (1), ‘sometimes’ (2), ‘often’ (3), and ‘every day or almost every day’ (4). Besides a total CPQ score, each domain can be rated separately. Furthermore, the OASIS was assessed. The OASIS is also an independent self-evaluation tool. It measures the childhood impact of external influences by asking questions concerning their perceptions of others and themselves, as well as about their previous behaviour related to the appearance of their teeth (Mandall et al., 1999). Therefore, children had to score five questions on a seven-point Likert scale (Figure 1). The scores for all questions were summed to provide an overall oral aesthetic impact score as perceived by each child (Flores-Mir et al., 2004; Bourne et al., 2012). The aesthetic self-perception of the own dentition was measured by the AC of IOTN: children were asked to identify which photograph in a series of 10 most closely matched the appearance of their anterior teeth.
Oral aesthetic subjective impact scale.
Clinical examination by calibrated orthodontists in training, supervised by one professor (certified for IOTN DHC and AC in the UK in 1993), was undertaken to assess the normative orthodontic treatment need. Both DHC and AC of IOTN were recorded.
Statistical analysis
All analyses have been performed using SAS software, version 9.2 of the SAS System for Windows, Copyright © 2002 SAS Institute Inc. SAS and all other SAS Institute Inc. product or service names are registered trademarks or trademarks of SAS Institute Inc., Cary, North Carolina, USA.
Spearman correlations were used to evaluate the relation between continuous/ordinal variables. Mann–Whitney U-tests were used to assess differences between two groups (gender). The agreement between the treatment need (AC of IOTN) assessed by the expert and by the child was quantified by mean of the intra-class correlation coefficient obtained from a one-way random model [ICC (1)] (McGraw and Wong, 1996). A Bland–Altman plot with 95 per cent limits of agreement was also constructed. Signed-rank tests were used to compare paired scores.
No corrections for multiple testing were performed. Given the large set of verified relations, P-values were considered significant when smaller than 0.005. The sample size was an extension of the data set discussed in the article of De Baets et al. (2012). With 386 included subjects, this study had over 87.7 per cent power to detect a correlation coefficient as low as 0.20 when the null hypothesis was that r = 0 and α was set at 0.005.
Results
The distribution of children according to the normative treatment need assessed by IOTN is shown in Table 1. According to the AC of IOTN, only 38.3 per cent had moderate to high treatment need (scores 5–10), whereas treatment was required in 80.3 per cent of the patients when based on the DHC of IOTN (scores 3–5).
Distribution of children according to normative treatment need (DHC and AC of IOTN; n = 386).
| Grade* | Normative treatment need (IOTN) | |
|---|---|---|
| DHC | AC | |
| No/low | 76 (19.7%) | 238 (61.7%) |
| Moderate/high | 310 (80.3%) | 148 (38.3%) |
| Grade* | Normative treatment need (IOTN) | |
|---|---|---|
| DHC | AC | |
| No/low | 76 (19.7%) | 238 (61.7%) |
| Moderate/high | 310 (80.3%) | 148 (38.3%) |
AC, Aesthetic Component; DHC, Dental Health Component; IOTN, Index of Orthodontic Treatment Need.
*No/low need = DHC grades 1 and 2, AC grades 1–4; moderate/high need = DHC grades 3–5, AC grades 5–10.
Distribution of children according to normative treatment need (DHC and AC of IOTN; n = 386).
| Grade* | Normative treatment need (IOTN) | |
|---|---|---|
| DHC | AC | |
| No/low | 76 (19.7%) | 238 (61.7%) |
| Moderate/high | 310 (80.3%) | 148 (38.3%) |
| Grade* | Normative treatment need (IOTN) | |
|---|---|---|
| DHC | AC | |
| No/low | 76 (19.7%) | 238 (61.7%) |
| Moderate/high | 310 (80.3%) | 148 (38.3%) |
AC, Aesthetic Component; DHC, Dental Health Component; IOTN, Index of Orthodontic Treatment Need.
*No/low need = DHC grades 1 and 2, AC grades 1–4; moderate/high need = DHC grades 3–5, AC grades 5–10.
For the perceived treatment need measures (Table 2), percentages of treatment need according to the AC child, OASIS and CPQ OS domain were comparable with those of AC expert (range 25.7–41.7 per cent). Considering the other domains of CPQ, distributions of less than 15 per cent were observed in the cases of moderate to high self-perceived need.
Distribution of children according to perceived treatment need (CPQ, OASIS and AC child; n = 386).
| Grade* | Perceived treatment need | ||||||
|---|---|---|---|---|---|---|---|
| CPQ | OASIS | AC child | |||||
| Total | OS | FL | EW | SW | |||
| No/low | 363 (94%) | 225 (58.3%) | 356 (92.2%) | 334 (86.5%) | 374 (96.9%) | 266 (68.9%) | 287 (74.4%) |
| Moderate/high | 23 (6%) | 161 (41.7%) | 30 (8.4%) | 52 (13.5%) | 12 (3.1%) | 120 (31.1%) | 99 (25.7%) |
| Grade* | Perceived treatment need | ||||||
|---|---|---|---|---|---|---|---|
| CPQ | OASIS | AC child | |||||
| Total | OS | FL | EW | SW | |||
| No/low | 363 (94%) | 225 (58.3%) | 356 (92.2%) | 334 (86.5%) | 374 (96.9%) | 266 (68.9%) | 287 (74.4%) |
| Moderate/high | 23 (6%) | 161 (41.7%) | 30 (8.4%) | 52 (13.5%) | 12 (3.1%) | 120 (31.1%) | 99 (25.7%) |
AC, Aesthetic Component; CPQ, Child Perceptions Questionnaire; EW, emotional well-being; FL, functional limitations; OASIS, Oral Aesthetic Subjective Impact Scale; OS, oral symptoms; SW, social well-being.
*No/low need = total CPQ scores 0–37, OS CPQ scores 0–6, FL CPQ scores 0–9, EW CPQ scores 0–9, SW CPQ scores 0–13, OASIS scores 5–10, AC child scores 1–4; moderate/high need = total CPQ scores 38–148, OS CPQ scores 7–24, FL CPQ scores 10–36, EW CPQ scores 10–36, SW CPQ scores 14–52, OASIS scores 11–35, AC child scores 5–10. Higher CPQ and OASIS scores refer to worse OHRQoL.
Distribution of children according to perceived treatment need (CPQ, OASIS and AC child; n = 386).
| Grade* | Perceived treatment need | ||||||
|---|---|---|---|---|---|---|---|
| CPQ | OASIS | AC child | |||||
| Total | OS | FL | EW | SW | |||
| No/low | 363 (94%) | 225 (58.3%) | 356 (92.2%) | 334 (86.5%) | 374 (96.9%) | 266 (68.9%) | 287 (74.4%) |
| Moderate/high | 23 (6%) | 161 (41.7%) | 30 (8.4%) | 52 (13.5%) | 12 (3.1%) | 120 (31.1%) | 99 (25.7%) |
| Grade* | Perceived treatment need | ||||||
|---|---|---|---|---|---|---|---|
| CPQ | OASIS | AC child | |||||
| Total | OS | FL | EW | SW | |||
| No/low | 363 (94%) | 225 (58.3%) | 356 (92.2%) | 334 (86.5%) | 374 (96.9%) | 266 (68.9%) | 287 (74.4%) |
| Moderate/high | 23 (6%) | 161 (41.7%) | 30 (8.4%) | 52 (13.5%) | 12 (3.1%) | 120 (31.1%) | 99 (25.7%) |
AC, Aesthetic Component; CPQ, Child Perceptions Questionnaire; EW, emotional well-being; FL, functional limitations; OASIS, Oral Aesthetic Subjective Impact Scale; OS, oral symptoms; SW, social well-being.
*No/low need = total CPQ scores 0–37, OS CPQ scores 0–6, FL CPQ scores 0–9, EW CPQ scores 0–9, SW CPQ scores 0–13, OASIS scores 5–10, AC child scores 1–4; moderate/high need = total CPQ scores 38–148, OS CPQ scores 7–24, FL CPQ scores 10–36, EW CPQ scores 10–36, SW CPQ scores 14–52, OASIS scores 11–35, AC child scores 5–10. Higher CPQ and OASIS scores refer to worse OHRQoL.
Table 3 shows a certain amount of children perceiving moderate to high orthodontic treatment need, in contrast to the IOTN measurements of the expert. The percentages reflect distributions of children in relation to the total sample size. The greatest percentages of children experiencing treatment need, although assigned to no or low treatment need by the practitioner, were observed in the CPQ OS domain and the OASIS. Concerning age and gender, no differences were found within the DHC and AC of IOTN.
Distribution of children according to moderate/high perceived treatment need (CPQ, OASIS and AC child) in relation to normative treatment need (DHC and AC of IOTN; n = 386).
| Normative treatment need | Perceived treatment need (moderate/high)** | |||||||
|---|---|---|---|---|---|---|---|---|
| IOTN* | ||||||||
| CPQ | OASIS | AC child | ||||||
| Total | OS | FL | EW | SW | ||||
| DHC expert | No/low (n = 76) | 4 (1.0%) | 27 (7.0%) | 7 (1.8%) | 6 (1.6%) | 2 (0.5%) | 17 (4.4%) | 9 (2.3%) |
| Moderate/high (n = 310) | 19 (4.9%) | 134 (34.7%) | 22 (5.7%) | 47 (12.2%) | 11 (2.8%) | 103 (26.7%) | 90 (23.3%) | |
| AC expert | No/low (n = 238) | 10 (2.6%) | 98 (25.4%) | 13 (3.4%) | 23 (6.0%) | 7 (1.8%) | 58 (15.0%) | 33 (8.5%) |
| Moderate/high (n = 148) | 13(3.4%) | 63 (16.3%) | 17 (4.4%) | 30 (7.8%) | 6 (1.6%) | 62 (16.1%) | 66 (17.1%) | |
| Normative treatment need | Perceived treatment need (moderate/high)** | |||||||
|---|---|---|---|---|---|---|---|---|
| IOTN* | ||||||||
| CPQ | OASIS | AC child | ||||||
| Total | OS | FL | EW | SW | ||||
| DHC expert | No/low (n = 76) | 4 (1.0%) | 27 (7.0%) | 7 (1.8%) | 6 (1.6%) | 2 (0.5%) | 17 (4.4%) | 9 (2.3%) |
| Moderate/high (n = 310) | 19 (4.9%) | 134 (34.7%) | 22 (5.7%) | 47 (12.2%) | 11 (2.8%) | 103 (26.7%) | 90 (23.3%) | |
| AC expert | No/low (n = 238) | 10 (2.6%) | 98 (25.4%) | 13 (3.4%) | 23 (6.0%) | 7 (1.8%) | 58 (15.0%) | 33 (8.5%) |
| Moderate/high (n = 148) | 13(3.4%) | 63 (16.3%) | 17 (4.4%) | 30 (7.8%) | 6 (1.6%) | 62 (16.1%) | 66 (17.1%) | |
AC, Aesthetic Component; CPQ, Child Perceptions Questionnaire; DHC, Dental Health Component; FL, functional limitations; EW, emotional well-being; IOTN, Index of Orthodontic Treatment Need; OS, oral symptoms; OASIS, Oral Aesthetic Subjective Impact Scale; SW, social well-being.
*No/low need = DHC grades 1 and 2, AC grades 1–4; moderate/high need = DHC grades 3–5, AC grades 5–10.
**Moderate/high need = total CPQ scores 38–148, OS CPQ scores 7–24, FL CPQ scores 10–36, EW CPQ scores 10–36, SW CPQ scores 14–52, OASIS scores 11–35, AC child scores 5–10. Higher CPQ and OASIS scores refer to worse OHRQoL.
Distribution of children according to moderate/high perceived treatment need (CPQ, OASIS and AC child) in relation to normative treatment need (DHC and AC of IOTN; n = 386).
| Normative treatment need | Perceived treatment need (moderate/high)** | |||||||
|---|---|---|---|---|---|---|---|---|
| IOTN* | ||||||||
| CPQ | OASIS | AC child | ||||||
| Total | OS | FL | EW | SW | ||||
| DHC expert | No/low (n = 76) | 4 (1.0%) | 27 (7.0%) | 7 (1.8%) | 6 (1.6%) | 2 (0.5%) | 17 (4.4%) | 9 (2.3%) |
| Moderate/high (n = 310) | 19 (4.9%) | 134 (34.7%) | 22 (5.7%) | 47 (12.2%) | 11 (2.8%) | 103 (26.7%) | 90 (23.3%) | |
| AC expert | No/low (n = 238) | 10 (2.6%) | 98 (25.4%) | 13 (3.4%) | 23 (6.0%) | 7 (1.8%) | 58 (15.0%) | 33 (8.5%) |
| Moderate/high (n = 148) | 13(3.4%) | 63 (16.3%) | 17 (4.4%) | 30 (7.8%) | 6 (1.6%) | 62 (16.1%) | 66 (17.1%) | |
| Normative treatment need | Perceived treatment need (moderate/high)** | |||||||
|---|---|---|---|---|---|---|---|---|
| IOTN* | ||||||||
| CPQ | OASIS | AC child | ||||||
| Total | OS | FL | EW | SW | ||||
| DHC expert | No/low (n = 76) | 4 (1.0%) | 27 (7.0%) | 7 (1.8%) | 6 (1.6%) | 2 (0.5%) | 17 (4.4%) | 9 (2.3%) |
| Moderate/high (n = 310) | 19 (4.9%) | 134 (34.7%) | 22 (5.7%) | 47 (12.2%) | 11 (2.8%) | 103 (26.7%) | 90 (23.3%) | |
| AC expert | No/low (n = 238) | 10 (2.6%) | 98 (25.4%) | 13 (3.4%) | 23 (6.0%) | 7 (1.8%) | 58 (15.0%) | 33 (8.5%) |
| Moderate/high (n = 148) | 13(3.4%) | 63 (16.3%) | 17 (4.4%) | 30 (7.8%) | 6 (1.6%) | 62 (16.1%) | 66 (17.1%) | |
AC, Aesthetic Component; CPQ, Child Perceptions Questionnaire; DHC, Dental Health Component; FL, functional limitations; EW, emotional well-being; IOTN, Index of Orthodontic Treatment Need; OS, oral symptoms; OASIS, Oral Aesthetic Subjective Impact Scale; SW, social well-being.
*No/low need = DHC grades 1 and 2, AC grades 1–4; moderate/high need = DHC grades 3–5, AC grades 5–10.
**Moderate/high need = total CPQ scores 38–148, OS CPQ scores 7–24, FL CPQ scores 10–36, EW CPQ scores 10–36, SW CPQ scores 14–52, OASIS scores 11–35, AC child scores 5–10. Higher CPQ and OASIS scores refer to worse OHRQoL.
For the perceived treatment need outcomes, girls tended to have higher scores than boys, but only significant (P = 0.001) for the CPQ EW domain; mean = 5.1, median = 3 (IQR = 1–8) versus mean = 3.1, median = 2 (IQR = 0–5), respectively. So girls experienced a lower OHRQoL than their male peers.
As it comes to age significant, but weak correlations were found with the OASIS scores (ρ = 0.20, P < 0.001) and with the AC child (ρ = –0.16, P = 0.002).
Relation between normative and perceived treatment need
Table 4 includes the Spearman correlation coefficients between the normative and perceived treatment need measures. The higher the normative treatment need (AC of IOTN), the higher the perceived treatment need except for the CPQ OS domain (P > 0.005). Although these correlations exist, the magnitude is weak (maximum ρ = 0.37 for the AC child). For the DHC of IOTN, only a relation was found with the AC child (ρ = 0.20, P = 0.0001).
Correlation between perceived treatment need (CPQ, OASIS and AC child) and normative treatment need (DHC and AC of IOTN).
| Perceived treatment need | Normative treatment need (IOTN) | |
|---|---|---|
| DHC expert | AC expert | |
| CPQ total | 0.07 (P = 0.1809) | 0.21 (P < 0.0001)* |
| CPQ OS | −0.04 (P = 0.4581) | 0.08 (P = 0.1160) |
| CPQ FL | 0.05 (P = 0.3528) | 0.16 (P = 0.0015)* |
| CPQ EW | 0.12 (P = 0.0226) | 0.23 (P < .0001)* |
| CPQ SW | 0.09 (P = 0.0679) | 0.16 (P = 0.0012)* |
| OASIS | 0.12 (P = 0.0197) | 0.21 (P < 0.0001)* |
| AC child | 0.20 (P = 0.0001)* | 0.37 (P < .0001)* |
| Perceived treatment need | Normative treatment need (IOTN) | |
|---|---|---|
| DHC expert | AC expert | |
| CPQ total | 0.07 (P = 0.1809) | 0.21 (P < 0.0001)* |
| CPQ OS | −0.04 (P = 0.4581) | 0.08 (P = 0.1160) |
| CPQ FL | 0.05 (P = 0.3528) | 0.16 (P = 0.0015)* |
| CPQ EW | 0.12 (P = 0.0226) | 0.23 (P < .0001)* |
| CPQ SW | 0.09 (P = 0.0679) | 0.16 (P = 0.0012)* |
| OASIS | 0.12 (P = 0.0197) | 0.21 (P < 0.0001)* |
| AC child | 0.20 (P = 0.0001)* | 0.37 (P < .0001)* |
AC, Aesthetic Component; CPQ, Child Perceptions Questionnaire; DHC, Dental Health Component; EW, emotional well-being; FL, functional limitations; IOTN, Index of Orthodontic Treatment Need; OASIS, Oral Aesthetic Subjective Impact Scale; OS, oral symptoms; SW, social well-being.
*Correlation significant (P < 0.005).
Correlation between perceived treatment need (CPQ, OASIS and AC child) and normative treatment need (DHC and AC of IOTN).
| Perceived treatment need | Normative treatment need (IOTN) | |
|---|---|---|
| DHC expert | AC expert | |
| CPQ total | 0.07 (P = 0.1809) | 0.21 (P < 0.0001)* |
| CPQ OS | −0.04 (P = 0.4581) | 0.08 (P = 0.1160) |
| CPQ FL | 0.05 (P = 0.3528) | 0.16 (P = 0.0015)* |
| CPQ EW | 0.12 (P = 0.0226) | 0.23 (P < .0001)* |
| CPQ SW | 0.09 (P = 0.0679) | 0.16 (P = 0.0012)* |
| OASIS | 0.12 (P = 0.0197) | 0.21 (P < 0.0001)* |
| AC child | 0.20 (P = 0.0001)* | 0.37 (P < .0001)* |
| Perceived treatment need | Normative treatment need (IOTN) | |
|---|---|---|
| DHC expert | AC expert | |
| CPQ total | 0.07 (P = 0.1809) | 0.21 (P < 0.0001)* |
| CPQ OS | −0.04 (P = 0.4581) | 0.08 (P = 0.1160) |
| CPQ FL | 0.05 (P = 0.3528) | 0.16 (P = 0.0015)* |
| CPQ EW | 0.12 (P = 0.0226) | 0.23 (P < .0001)* |
| CPQ SW | 0.09 (P = 0.0679) | 0.16 (P = 0.0012)* |
| OASIS | 0.12 (P = 0.0197) | 0.21 (P < 0.0001)* |
| AC child | 0.20 (P = 0.0001)* | 0.37 (P < .0001)* |
AC, Aesthetic Component; CPQ, Child Perceptions Questionnaire; DHC, Dental Health Component; EW, emotional well-being; FL, functional limitations; IOTN, Index of Orthodontic Treatment Need; OASIS, Oral Aesthetic Subjective Impact Scale; OS, oral symptoms; SW, social well-being.
*Correlation significant (P < 0.005).
Agreement between AC expert and AC child
The treatment need (AC of IOTN) as evaluated by the child is on average lower than the treatment need evaluated by the expert. This mean difference is small (mean difference = 0.38, P = 0.001), but with a large variability (SD = 2.40) resulting in children overestimating and in children underestimating their problem. Only 43.5 per cent of the children consistently (i.e. maximum 1 grade of difference with the practitioner) rated their dentition. The Bland–Altman plot (Figure 2) visualizes this low degree of agreement with wide 95 per cent limits of agreement (–4.3, 5.1), ICC = 0.38; 95 per cent CI: 0.29, 0.46.
Agreement (Bland–Altman plot) between AC expert and AC child.
Discussion
In this study, the group of children considered to have orthodontic treatment need (moderate to high) according to DHC measurements was much larger than the group based on AC expert scores, conform the study of Nobile et al. (2007). The reason for this difference is the registration of two different attributes: the DHC is based on occlusal characteristics, whether the AC determines treatment need purely on aesthetic grounds (Brook and Shaw, 1989). An even larger discrepancy was seen between the distribution of DHC of IOTN (80.3 per cent) and that of most of the CPQ domains (3.1–13.5 per cent). This could be indicating a low impact of the children’s dentition on their daily lives, but it should be noted that although the CPQ appears to reflect subjects’ concern about malocclusions and perceived need for orthodontic treatment, the CPQ does not reveal the subject’s perception of the actual cause of any of the impacts which are scored (Kok et al., 2004). This could explain as well on the contrary the high percentage in the OS domain (41.7 per cent) since the specific questions involved were highly related to other common oral health conditions, more than to the subjects’ malocclusion (i.e. ‘In the past 3 months, how often have you had bleeding gums?’ or ‘In the past 3 months, how often have you had bad breath?’).
On the other hand, the measures clearly mentioning the appearances of one’s dentition in the questionnaire/images, OASIS and AC child, had a distribution comparable with that of AC expert (±30 per cent) in assessing treatment need. It confirms that people seek and undergo orthodontic treatment not because of the anatomic irregularities per se or to prevent the destruction of tissue within the oral cavity, but because of the consequences of the aesthetic impairment caused by malocclusion (Burden, 1995).
For DHC of IOTN, no relation was found between any of the perceived treatment measures, except for the AC child (P = 0.0001). For AC of IOTN on the other hand, significant but weak correlations with all of the perceived treatment need measures were recorded (ρ = 0.16–0.37, P < 0.005), except for the CPQ OS domain (P > 0.005). These results are according to previous findings of Kok et al. (2004) and in line with our preliminary study group investigated by De Baets et al. (2012). Although a relationship was found between normative and perceived treatment need, the weakness of it indicates the presence of some children missing the boat on orthodontic treatment if solely based on normative treatment need indices. This was illustrated by the percentages in Table 3 with OASIS detecting most of those children. However, it must be noted that in this study population it concerns only a rather small group of patients. The discrepancies highlighted in this study between clinical normative need and child’s perceived need are supported by the findings of de Oliveira and Sheiham (2003) and de Oliveira et al. (2008). The authors found that a certain percentage of children who were assessed to have no or low orthodontic treatment need by the IOTN index did experience oral health impact [measured by the CPQ11–14 and the Child-OIDP (Oral Impacts on Daily Performances)].
The explanation for this could be found in the fact that some children have remarkable levels of concern for the most minor anomalies, and, paradoxically, others are tolerant of severe occlusal problems. More adolescents with good aesthetic occlusion who feel dissatisfied with their teeth have been reported (Howitt et al., 1967; Lewit and Virolainen, 1968; Onyeaso and Sanu, 2005). Therefore, it is reasonable to assume that the relationship between reported self-perceived treatment need and malocclusion is most likely moderated by other factors. Studies in the medical literature have stressed the importance of innate psychological attributes, such as self-esteem (SE), in predicting the effect of health conditions on the quality of life (Foltz, 1987; Katz et al., 1995). SE can be defined as the perception of one’s own ability to master or deal effectively with the environment and is affected by the reactions of others towards an individual (Tung and Kiyak, 1998). The higher the SE, the higher the self-perceived level of the attractiveness of the face or positive feelings towards the dentofacial region. Indeed, in the study of De Baets et al. (2012), a significant relationship between SE and OHRQoL measured by CPQ was found. However, SE did not play a role as moderator on the relationship between normative treatment need and OHRQoL. The Wilson–Cleary model provides a useful framework to investigate the relation between orthodontic treatment need and OHRQoL and the potential moderating role of several other factors: biological variables, symptom status, health functioning, general health perceptions, environmental, and individual (e.g. SE) factors (Wilson and Cleary, 1995).
Previous studies have shown that laypeople tend to have a less critical perception of the same malocclusions compared with professionals (Shaw et al., 1975; Prahl-Andersen, 1978; Stenvik et al., 1997). The AC of IOTN evaluated by the child similarly did correspond poorly with the scores of the practitioner, underestimating their own malocclusions. The low agreement can be explained by two different pathways. In a first explanation, we could maintain the fact that the AC of IOTN effectively reflected the child’s motivation and concern for orthodontic treatment, being totally different from the practitioner’s judgement. Indeed, in the past it has been shown that the AC child is of some value in assessing perceived treatment need (Yeh et al., 2000). However, in the study of Grzywacz (2003), there was a significant agreement in the AC between the professional ratings and the children’s assessments. Approximately, twice as much children consistently rated their malocclusion in comparison with our study population (84.5 versus 43.5 per cent). Anyhow, more than half of those children were currently undergoing or had previously undergone orthodontic treatment, which means that the largest part could be assigned to the no or low treatment need category; this group showing not so much variation in the four first photographs on the AC of IOTN colour scale as the teeth are quite well aligned in all of them. Mandall et al. (1999), on the other hand, had similar results to our study group; also approximately half of the children (54 per cent) agreed with the examiner regarding aesthetic treatment need. This study group was conform to our population; much larger (n = 334 versus 84) and not influenced by treatment as every child already received orthodontic treatment was removed from the analyses. This leads us to another and more reasonable explanation for the poor agreement: the age and as a result the stage of dental development of the children. Indeed, in the late mixed or early permanent dentition, the occlusion exhibits some characteristic traits that are reflected in the AC photographs. However, the essence of the construction of the AC of IOTN is the overall aesthetic aspect and not to compare tooth morphology (Holmes, 1992; Birkeland et al., 1996). This fact may have had a bearing on the outcome of the assessment of aesthetics by children who were not able to distinguish normal development irregularities and malocclusions. There was effectively a negative correlation between age and AC child (ρ = –0.16, P = 0.002). This means that younger children tended to categorize themselves worse-off than older ones, the youngest being completely in the late mixed dentition stages. These difficulties were also identified in the study of Flores-Mir et al. (2004), however, dealing with a young–adult population.
The lack of agreement might also be partially due to the likely presence of measurement error in both the child as in the expert measurements. Indeed, when measurements do not show perfect reliability, the correlation between them will be attenuated.
Conclusions
Perceived treatment need as assessed by the CPQ and the OASIS correlated only weakly with the normative orthodontic treatment need measured by the AC of IOTN. Although a correlation was found, the agreement between the AC of IOTN of the examiner and the child was very poor, suggesting a difficulty for the child in evaluating the overall aesthetic aspect of its own malocclusion.
For the DHC of IOTN, only a relation was found with the AC child. Given the discrepancy between normative and perceived treatment need found in this study, the commonly used IOTN as a clinical assessment tool for orthodontic treatment need should be reinforced by OHRQoL measures, like the OASIS, expressing patients’ perceived treatment need.
References


{kind=link}